
In this big pinch, I’m going to describe some of my PhD work that looked at attention in pain, as a concrete example of the research process to understand why pain makes it hard to think.
Words in blue bold text are research jargon; I’ll define these as we go along.
Science is a team effort in many ways. You work with other researchers, build on the findings of many other researchers before you, and ask for participants to participate in your experiments.
For this research, published in 2020, I worked with Dr Gina Grimshaw, Dr Ron Fischer (my primary and secondary PhD supervisors respectively) and Dr Amy Walsh.
I am very grateful to all the people, with and without chronic pain, who volunteered their energy and time for my experiments. Psychology research cannot happen without research volunteers. The methods I use involve looking at behavioural responses to tasks (accuracy and response time). You cannot make inferences from one person doing one task. Rather, you need many people doing the task multiple times to get stable estimates of the phenomena of interest.
I do not take this volunteering of time and energy lightly. Everyone has things going on in their lives, and they give some of their day to us as researchers.
For this pinch, I draw on writing from my PhD1 and from the article published in Clinical Psychological Science2.
Research question
In research we have a question we are trying to work towards answering. That research question in Psychology could be about an aspect of the mind (e.g., memory), the brain (e.g., the hippocampus), and/or behaviour (e.g., following a route). We want to understand what is driving some aspect of human activity.
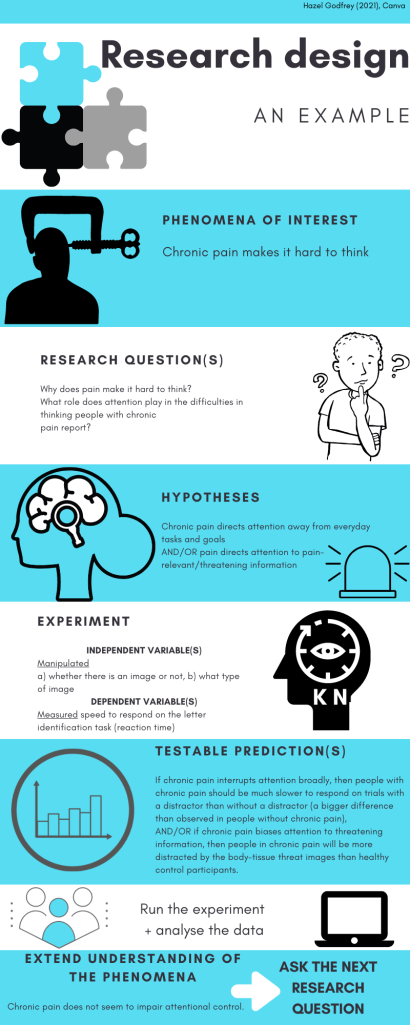
My broad research question was “why does pain make it hard to think?“. This question was first planted in my mind in the pain management programme I attended. It is a huge and complicated question, and not something that’s going to be answered with one experiment! My narrower research question about the mind in pain, was “what role does attention play in the difficulties in thinking people with chronic pain report?“.
As well as your collaborators and participants you are also drawing on work of scientists before you. Research doesn’t build from nothing. Other scientists have published studies on attention in chronic pain; what had they established? There were two main groups of findings on the impact of pain on attention. 1) attention was “interrupted” by pain. 2) people with chronic pain showed greater attention towards information relevant to pain and away from information not-relevant to pain. These findings led me to design research to test between two hypotheses about how the mind controls attention in pain.
Hypotheses
Hypotheses are statements that describe how you think the phenomena of interest works.
In the cognitive psychology theories I drew on, attention is seen as a finite thing. There’s only so much of it available for us to focus on our day-to-day tasks and goals. Under this view, in chronic pain, attention is directed to the pain sensation and away from current tasks and goals. This leads to broad cognitive deficits; difficulties in thinking. I referred to this view as the deficit-view of attention in pain (hypothesis 1). One way to look for deficits is to compare how fast people with, and without, chronic pain respond on tasks. That is, reaction time.
However, there was that other set of findings – on attentional bias. An attentional bias means a tendency to attend to certain kinds of information over others. Some experiences can act as motivators (e.g., hunger, thirst, pain, itch) that makes it easier to process certain types of information (for example, things that are related to threat) and impairs processing of other, less relevant, information (such as, our current task).
The enhancement of processing some types of information is called an attentional bias. An attentional bias to pain related information has been observed in people with chronic pain, suggesting that attention is motivated towards information in the environment that is pain related, and away from information that is not. Such an attentional bias may contribute to the cognitive deficits observed with tasks using neutral information (motivated attention view; hypothesis 2).
The stimuli, or information in the experiment could be anything, something you perceive with your senses. I focused on visual attention with visual stimuli both related to pain and neutral (e.g, images).
Testable predictions
In testing for evidence of the deficit-view and motivated attention view of attention, we needed to use a method to observe attention and state testable predictions for the hypotheses. Testable predictions are basically “if…then” statements. If we observe x then this is support for y hypothesis. Again we drew on work by others. We used a task that allows you to infer distraction by different kinds of information.
Specifically, the task examined how people can be distracted by emotional images. Emotional stimuli are important for our survival, and are usually given priority by our perceptual and attentional systems. However, sometimes it is important to ignore emotional stimuli so that we can achieve other goals; I need to ignore the ice cream truck so I can get my work done. We asked the participants to do a simple perceptual task (looking for a letter) and measured how quickly they responded; their reaction time (the dependent variable = what I measured).
The independent variables in experiments are what the researcher is manipulating. We manipulated a) whether an image was presented at the same time as the letters, and b) the nature of the image. On some trials, a distracting picture was also presented which could be either convey a pain-relevant body-tissue threat (mutilations or injuries), or neutral (people doing day to day things).
Generally, we expected, based on previous research with this emotional distraction task, that threatening images would be more distracting than neutral images; and confirmed that in a pilot experiment (a small experiment to prepare for the main experiment, to check things are working as we expect them to; like a pilot episode for a TV show). People were slower to respond to the letter task when there was a threatening image present than when a neutral image was present, reflecting greater distraction by the threatening images.
Our testable prediction for the deficit-view was: if chronic pain interrupts attention broadly, then people with chronic pain should be much slower to respond on trials with a distractor than without a distractor (a bigger difference than observed in people without chronic pain). Our testable prediction for the motivated attention view was: if chronic pain draws attention to threatening information, then people in chronic pain will be more distracted by the body-tissue threat images than people not in chronic pain.
However, that isn’t what we found. Our hypotheses were not supported. We observed that there was an attentional bias towards the body-tissue threat information; people were more distracted (slower to respond to the letter) by body-tissue threat images than neutral images.
However, when we compared the size of the attentional bias to body-tissue threat images in people with and without chronic pain, we found no difference between the two groups. This suggests that chronic pain does not motivate attention towards signals of threat to body-tissue any more so than is observed in people without chronic pain. Rather, an attentional bias towards images of body-tissue threat is present in groups of people with and without chronic pain.
We did include other tasks and questionnaires that I won’t describe in detail here. Overall, although chronic pain does not seem to impair peoples’ ability to focus when distractions were present, participants with chronic pain reported feeling like they had less attentional control and that they paid more attention to pain than participants without chronic pain. On tasks where we measured how long it took to make a response, participants in chronic pain were slower to respond than participants without chronic pain.
These findings together suggest that something has changed in how people with chronic pain complete these attention tasks, but from my PhD work we now know that this is likely not due to an enhanced attentional bias to pain-relevant information. It is likely not due to an impairment in attentional control. Perhaps another process such as early perceptual processing, or memory, or decision making, underlies cognitive difficulties in chronic pain.
In summary, the data do not support either the deficit-view or motivated attention view of attentional control in chronic pain. While completing my thesis I also carefully reviewed other research on how pain affects cognition. While it is commonly experienced that pain ‘makes it hard to think’, there are many studies that don’t find these deficits on performance of tasks, and so it is not clear what aspects of thinking might be affected. In terms of clinical use to reduce difficulties in thinking, we do not yet understand enough about how pain affects cognition. More research is first needed to identify potential mechanisms by which pain affects cognition. Once we understand the underlying mechanisms, then we can develop targeted strategies to help people in chronic pain manage their difficulties in thinking.
In a next pinch I’ll write about my experience of doing research to further understanding of pain as someone with pain.
1. Godfrey, H. K. (2017). A role for attentional bias in cognitive deficits in chronic pain? [Doctoral thesis, Victoria University of Wellington]. http://researcharchive.vuw.ac.nz/handle/10063/6814
2. Godfrey, H. K., Walsh, A. T., Fischer, R., & Grimshaw, G. M. (2020). The role of attentional control in cognitive deficits associated with chronic pain. Clinical Psychological Science, 8(6), 1046-1053. https://doi.org/10.1177/2167702620925744

Such a good write up. You do amazing and carefully considered work!
LikeLike
Thanks Pete 🙂
LikeLike
Pingback: “You hurt too much”: pain, suffering, and stigma – Pinches of Pain